
 Abstract: The cascading collection of seemingly minor unfavorable elements during a particular commercial flight can often arouse little notice because there may be no collective safety measuring system or metric to assemble disparate elements. However, just as the story of “the straw that breaks the camel’s back[1]” informs us, flight crew members facing unusual accumulations of circumstances during flight operations from aircraft automation systems, the weather, airfield navigation equipment, human factors, their passengers and payloads, and at times even local and international politics can at times be overwhelmed. Without a metric to determine how far from normal reality a particular flight has deviated, the flight crew, the dispatchers, air traffic control and supervisory personnel in regulatory positions and corporate administration may not have an effective tool to detrrmine when, where and how to establish additional procedures and limitations to address any level of significant deviations from normal reality or as we have label this, the rise of Unusuality.
Abstract: The cascading collection of seemingly minor unfavorable elements during a particular commercial flight can often arouse little notice because there may be no collective safety measuring system or metric to assemble disparate elements. However, just as the story of “the straw that breaks the camel’s back[1]” informs us, flight crew members facing unusual accumulations of circumstances during flight operations from aircraft automation systems, the weather, airfield navigation equipment, human factors, their passengers and payloads, and at times even local and international politics can at times be overwhelmed. Without a metric to determine how far from normal reality a particular flight has deviated, the flight crew, the dispatchers, air traffic control and supervisory personnel in regulatory positions and corporate administration may not have an effective tool to detrrmine when, where and how to establish additional procedures and limitations to address any level of significant deviations from normal reality or as we have label this, the rise of Unusuality.
Captain David Williams and his writing partner Captain Paul Miller have developed a simple measuring tool, a comprehensive system and an easy to use metric to aid flight crew members, dispatchers and others involved in commercial flight operations to determine when the accumulation of seemingly unrelated elements begins to form a major hazard to safety. The metric is in the form of a checklist and addresses the flight crew, the aircraft, the natural environment and the automated flight environment. It provides guidance when to consider alternative procedures from an aggregate of unusual elements labeled “Unusuality.” When the deviation from normality is contrasted with the normal reality, or normality, the metric become a clear tool comprehensible by the layman and professional alike, this being an important tool for communications, to bring everyone onboard quickly. Why? Every airline and every situation of combined factors will be different and particular. That is why these combinations often are not noticed until after the mishap investigation begins, if in fact a mishap has occurred, as the safety record shows it often has.
The take away from this paper will be a detailed checklist to allow all involved in commercial flight operations to identify hazards of Unusuality, and take action to prevent a costly mishap.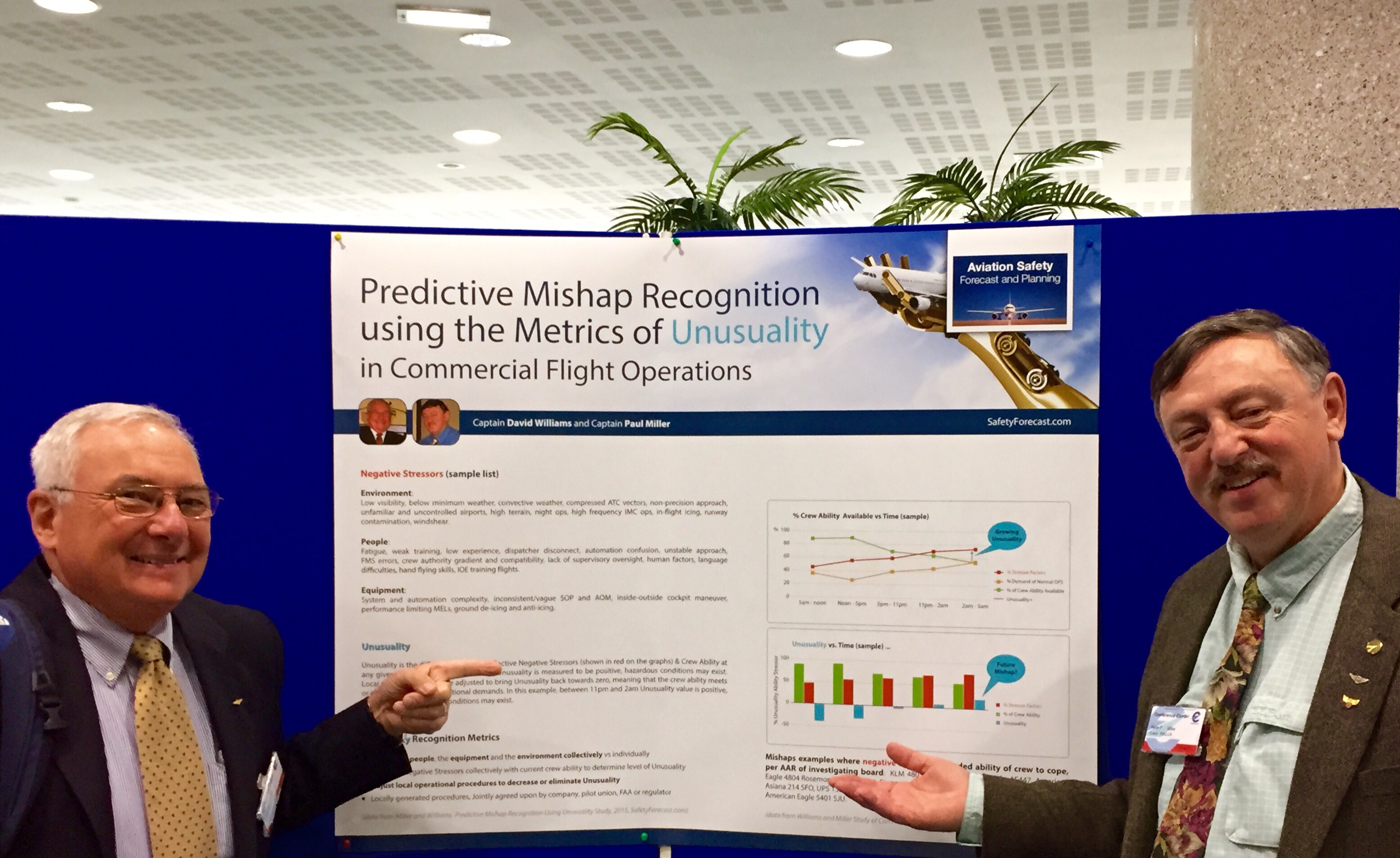
Question: Can we use what we already know to prevent commercial aviation mishaps?
National Transportation Safety Board member Robert Sumwalt recently stated “We want to get the facts before we start making judgments.”[2] He also stated that the NTSB looks at three major areas during a mishap investigation: the environment, the people and the machine.[3]
If the facts were in existence prior to a mishap, that is, that they were able to be discovered by the NTSB as facts, after the mishap and provide the NTSB with the factual cause(s) of the mishap, could these same facts, be knowable at the time of the mishap? Furthermore, since aviation mishaps are very fluid and seem to have a very fast moving time line of factual events[4], could the facts that were later determined to have been the cause(s) of the mishap, be known, both as they were occurring and, if in existence prior to a mishap, be known and recognizable prior to the mishap?
If the facts that cause a mishap can be known and recognized prior to the mishap, can we create a method, a metric of recognizing these facts as things-about-to-become-causes[5] for the mishap, prior to the mishap?
If the methodology that the NTSB uses to determine these causes after the mishap, is valid and continues to be validated by each mishap investigation, could we not adapt this methodology into some form of recognition procedure, a metric to identify these causes, as they factually exist, prior to the mishap? If we can adapt this methodology to create a procedure to recognize these facts as things-about-to-become-causes could we create a metric, that each airline could adapt, to serve as their own local mishap prevention flight safety management procedure tool, since each airline would and should know their own environment, people and equipment the best?[6]
If the various “things-about-to-become-causes” were relabeled to be “Negative Stressors”[7] could they be given a vector value, that is both a size value and a direction value, in a manner similar to false color imaging used by radio astronomical observers?[8]
If we could give these Negative Stressors vector values, could we quantitatively sum these vectors with other similarly derived vector values for such things as crew ability and normal operational demands and then plot them graphically?
If by plotting graphically the negative stressors along with normal operational demands and crew abilities, could we get a graphical understanding of rare circumstances where the vectors of negative stressors exceeds the crew ability and the normal operational demand curves? If we could get a graphical understanding of such areas of exceedance, could we relabel these areas as Unusuality, that is, areas on the graph where the collective level of negative stressor vectors far exceeds any level of expectation of normal operational demand, or normalcy for that aircrew?
If we can calculate and plot Unusuality by referencing the facts after a mishap, facts that were all known and in existence before the mishap, could we calculate and plot Unusuality prior to a mishap?
If we could calculate and plot Unusuality prior to a mishap, could any airline then use this recognition of Unusuality to adjust that airline’s standard operating procedures as a method of intervening ahead of time to prevent a mishap from occurring in the first place?
Could commercial airline mishaps be prevented by better understanding, recognizing and acting locally on occurrences of Unusuality?
As the various operational elements and flight crew dynamics combine and integrate during a flight’s duration, the cumulative effects can create significant hazard to the operational safety of that flight. By analyzing aircraft After Accident Reports (AAR) from various governmental organizations and identifying both the subjective and qualitative elements gleaned from the contemporary AAR’s data base, a demonstrated pattern of operational detriments can be determined as stressors against crew capability and thereby addressed and mitigated. With current flight crew training and checking programs, agency regulatory oversight and redundant aircraft systems, rarely does a single negative element encountered during a flight create an anomaly of sufficient proportion that it will result in an accident. Conversely, when several negative elements or stressors exist, are experienced or are encountered, the effects can be cumulative and translate into a cumulative flight hazard, that may exceed the individual threat of each negative stressor and exceed the crews’ ability to cope with, handle or to otherwise, using trained standard operating procedures, successfully complete the flight. As positive elements can interact and combine to create a positive synergy[9] with an improved and safer operating environment, the converse effect of negative elements, we postulate, could create a negative synergy[10] and is of an equal but negative dynamic. The cumulative negative stressors could overwhelm a flight crew, rendering them ineffective and unable to extricate themselves from the dangerous and deteriorating situation in a timely manner.
While the effect of each negative stressor may be considered of limited significance, the combined effects of such multiple elements becomes apparent in retrospect, as noted in After Accident Reports[11]. If flight crews and oversight agencies can recognize the compounding negative synergy of such stressors ahead of time by some form of a observatory measuring metric, an emerging threat can be recognized, anticipated, mitigated or avoided. The area that we are studying is the difference between a particular crews’ ability to handle hazards, unexpected events and failures and the level of accumulation of these hazards, unexpected events and failures. Thus, as a particular airline training and procedures program rises to be more comprehensive, the difference could be reduced. As the involvement of more of the management team, such as dispatch, meteorology, scheduling, maintenance and chief pilot’s office, increases, the difference could, once again decrease. As a crew is more mentally sharp due to rest[12] and diminishment of factors of mental distraction, their capability could increase substantially and thus the difference would be reduced. We define the difference between the accumulated level of negative stressors and the current crews ability to cope successfully with them in total, as the level of Unusuality. Again, it is not any single factor that we are addressing, but rather the difference between the sum total negative stressors and the sum total ability of that crew at that time to cope with all of them in a timely and successful manner. Unusuality may be important to understand since very often post accident reviews by boards and later airline procedure writers and training program writers may focus on one causal element at a time. For example, the ATSB (investigating mishap board) cited the crew’s delay to dump fuel to landing weight as a itemized factor, leading the reader to believe that if they only had not delayed their approach to landing , that this mishap might have been averted. But the crew of Swiss Air 111 was dealing simultaneously with an overwhelming number of factors, all at the same time. They were not startled, they were overwhelmed. They were dealing with night, over the water, severe and unknown electrical malfunction that was rapidly escalating, a design and engineering flaw within the aircraft’s post production modification, for which documentation and trained non-normal procedures were ineffective, and a heavy aircraft, soon after take off, fueled for a transatlantic crossing, at much heavier than normal landing weight. The crew was well trained and qualified; however, the sum total of negative stressors appears to have overwhelmed the crew’s ability to react timely and successfully. [13] The level of Unusuality was so great in this case that it prevented a successful outcome. Yet, the design and engineering flaw was detectible by mishap investigators after the mangled wreckage was lifted from the ocean floor months after the mishap. Could not a quality assurance inspection have discovered the same flaw prior to the mishap? Could the crew have dived as rapidly as possible to the end of a runway at nearby Nova Scotia, landed heavy and omitted the attempt at fuel dumping to standard landing weight? Comments invoking this procedure were made afterwards[14]. Could not similar conclusions have been reached by local procedures writers at the airline, the manufacturer or the regulator prior to a mishap occurring? We believe that there is something to be learned.
To support this hypothesis, the authors have reviewed data related to negative elements from multiple National Transportation Safety Board (NTSB) Aircraft Accident Reports (AAR) and ICAO AAR from 1990-2013 for documented accident research, both in the USA and Europe. These negative stressors are then evaluated for a numerical cumulative causal relationship. If these negative elements are cumulative, we postulate that there may exist more than just an anecdotal relationship.
This paper postulates that the safety of individual flights can be improved if flight crew members and the assigned flight dispatcher are knowledgeable of these negative stressor elements and the potential negative cumulative effect. They then can take locally generated procedural actions and other timely and appropriate timely mitigation measures to either eliminate or reduce those elements and prevent a mishap from occurring.
We postulate that if cumulative negative effects can contribute to an accident, then the corollary exists for the cumulative “positive element” synergy to exist that contributes to an improved safety effectiveness by the flight crew. Possible examples of this postulated “positive element synergy” might be an explanation for several remarkable accidents where flight crew interactions contributed to a more successful outcome than might have been expected. Two examples might be further evaluated for such positive synergistic effect; United Airlines Flight 232 Sioux Falls SD, July 1989 and USAir Flight 1549, January 15, 2009, the successful Airbus A320 ditching, the “Miracle on the Hudson”.
End of Introduction.

<<<<<<<<<<<<<<<<<<<<<<<<<<>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
“The best-laid plans of mice and men / Often go awry” from To a Mouse, by Robert Burns[15]
<<<<<<<<<<<<<<<<<<<<<<<<<<<<<>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>
Board Determined Causal Factors: The accidents investigated by the National Transportation Safety Board (NTSB) list the Probable Cause and Contributing causal factors.[16] Many of these principle Probable Cause factors have been cited in multiple accidents.[17] Significant efforts have been enacted by all major stakeholders in the aviation, safety industry and regulatory agencies to correct these causal factors with improved training, better equipment, and governing regulations.[18] Efforts to identify and correct potential causes of future accidents have met mixed results although the overall accident rate has significantly decreased during these past five decades.[19] Repetitive accidents with the same Probable Cause, however continue to occur. Today, the chances of being in a commercial airline accident are statistically very low, one in a million or less[20]. However, we have found that several major elements exhibit a recurring frequency and are particularly problematic despite significant and continual efforts to correct, mitigate and prevent such occurrences. Major programs and technical advances such as improved flight crew training standards, onboard flight weather radar, Traffic Collision Avoidance System (TCAS II/III), Enhanced Ground Proximity Warning System (EGPWS), improved navigation equipment, airport taxiway and runway markings and lighting have directly aided flight safety. Despite aircraft design improvements, industry, regulatory, employee efforts, improved flight crew training and advanced avionics, multiple causal factors, what we call negative stressors, continue to negatively impact safe operations. While these negative stressors are known, programs to mitigate these mishap causal elements, is not the total solution.
We define Unusuality as the difference between accumulated negative stressors and the crew’s ability to counter the cumulative effects of those negative stressors at any point in time. Other mishap prevention programs have met with mixed effectiveness, because they are often compared against an ideal, well rested crew, where most often, negative stressors are presented one at a time in typical FAR Part 121 training. [21]
But our study of multiple mishap board AARs has determined that virtually all mishaps result after an unusually high level and near-simultaneous or cascading presentation of negative stressors. In most cases, mishap board AARs did not list one singular negative stressor as the Probable and/or Contributing Cause. In stark contrast rather, virtually every mishap board listed an accumulative set of Probable and Contributing Causes. It is our argument that crews were in many, if not most cases overwhelmed by this accumulation of the negative stressors of all of Probable and Contributing Causes happening at that time, above and beyond their ability to react, cope and handle the accumulated causes. This overwhelming level of causes, as listed by the mishap investigation boards, that exceeds the crews’ ability is what we define as Unusuality. It is important to understand that Unusuality is not merely the accumulation of negative stressors as listed by mishap investigation boards as Probable and Contributing Causes. Rather, Unusuality is the difference between the overwhelming accumulation negative stressors and the crews’ ability to react successfully at that time. Part of the common confusion with this calculation is that not every crew performs at the same level. Due to teamwork, familiarity, a more developed skill set, a wider aeronautical education and training back ground, some people appear to be able to handle just about anything thrown at them. While they may use written SOP, the also may dip deep into a well of additional knowledge brought to work from off campus studies and training, personal ability and mental acuity possessed by few. The crew of United 232 that landed an DC-10 with no hydraulic power to operate flight controls used essentially their cooperative wits in place of SOP to bring the aircraft to the runway, saving 185 lives of the 296 persons onboard. [22]

If the Probable Cause is easily identified after the accident by investigative methods, why cannot methods be employed to identify Probable Causes before the accident occurs?
What is Unusuality as it applies to flight crews and the stressors that contribute to an aircraft accident? While the Probable Cause of an accident may be readily apparent, what other elements contributed to that accident and led that trained flight crew to a critical operational failure? Probable Causes and Contributing Causes leading to an accident we define as negative stressors. These negative stressors have a cumulative effect, not a singular effect. The cumulative effect of the negative stressors, and not just the causes considered singularly, that overwhelm the crew ability, may be the issue that needs to be understood. Again we define Unusuality as the difference between a particular crew’s ability to perform on a particular flight while influenced by the sum total of negative stressors encountered.
While it is beyond the scope of this paper to sufficiently quantify the stressors as they relate to Unusuality, it is an objective of the authors to have companies review and develop methods with their stakeholders (companies, pilot groups, safety officials, regulators, policy writers) to assess the stressors that impact their organization’s operations and to establish a working group to study the associated dynamics. When those specific stressors are identified and considered, a company specific metric can be designed and evaluated. While organizations may have similar stressors, one company may have reach the point of “Unusuality (cumulative stressors minus crew’s abilities at that time) while another company doing similar operations may NOT reach “Unusuality”. Different flight crews within the same company, because of individual abilities, use of SOP’s, refined CRM skills and previous training may NOT reach the point of “Unusuality”. Why do some crew members have higher skill levels than others? All crew members are required to pass the same check rides,
Consider USAir Flight 1549, the “Miracle on the Hudson” (bird strikes causing loss of both engines causing the subsequent ditching in the Hudson River[23]). Although most flight crews are hazarded by bird strikes, this aircraft’s flight crew effectively managed a double engine failure while at 2818 feet agl, performing multiple emergency QRH 2-crew “response, “confirm”, comply” procedures, multiple coordinated relight attempts, notifying the passengers to “brace for impact”, and configuring the aircraft for a successful dead-stick ditched landing, remarkably all within 3 minutes and 33 seconds.[24] For this crew to achieve this level of effective CRM and airmanship when confronted with multiple challenging stressors, yet not reach the point of “Unusuality” is most significant even to consider. Would other flight crews within that same company or any other airline, given the same circumstances, have been able to achieve this same level of performance?
What we are saying is that crew ability varies because of many factors. Some of these factors may be level of training as noted in our paper Training to Safety in Commercial Airline Operations. [25]
“Unusuality” metric is different for each operator. An airline operating under FAR part 121 with aircraft equipped with infrared runway detection heads up devices installed in the flight deck may be certified to operate down to a RVR of 600, while most similar carriers without that equipment may be limited to 1200 RVR.
Some airlines are so equipped and flight crews trained to permit full CAT IIIC operations with an RVR of 500. Sufficient equipping, maintenance and flight crew training is required for authorizing certification. The point of a concerning level of Unusualty where crew’s abilities to operate do not meet required operations levels would be different for each of these two air carriers although the stressors may be alike.
The Unusualty metric should prompt added attention by stake holders. Mitigation to provide for a safer operating margin would be postulated by those involved. Mitigations might include:
- Increased flight crew training in a specific recurring problematic stressor, such as fatigue (recognizing fatigue factors; possible flight schedules modifications; developing an improved company policy for calling in because of fatigue; increasing crew manning numbers; replacing a current crew with a reserve crew for the last flight of the sequence when marginal destination weather or airfield stressors exist (precision approach out of service, tailwind landing, icing conditions, severe weather enroute or at airport, etc.).
- Specific flight and duty day limitations for captains when performing Initial Operating Experience (IOE).
- Replacing a low time flight crew member with a more experienced member for a demanding approach or a particularly demanding airport.
NASA Ames Research Center Counter Measures Fatigue Studies[26] (footnote) evaluated flight crew performance and documented degradations from the optimum effectiveness even for experienced and well trained flight crews. Fatigue, a frequently present stressor directly degrades crew coordination, communications skills, procedural accuracy, alternatives planning, and visual perceptions. Because fatigue becomes consuming in the later stage of a crew’s duty time, the added demands placed on a flight crew, while not being necessarily obvious to the crew, becomes apparent in the post accident review. In this instance as the effects of fatigue accumulate, the level of Unusuality (the difference between the crew’s ability to sufficiently handle versus the unexpectancy of the cumulative stressors) actually increases during the flight, since Unusuality is the difference between the crew’s performed ability to counter cumulative stressors.
Flight crews encountering severe weather at the final stage of their scheduled duty day require their optimum performance. But because performance levels have decreased with fatigue (poor decision making, slowed reaction time, reduced vigilance, poor communications, instrument scan fixation, apathy, lethargy, mood swings, uncontrolled nodding off), they may not be able to meet operations in demanding conditions at their destination airport. The “unusuality” gap between their collective abilities and the cumulative stressors encountered may be exceeded. As instrument approach minimums are being reached, a flight crew may have mere seconds to detect the runway environment, establish orientation to that runway, transition the aircraft to the landing and then complete the roll-out. There are few other maneuvers requiring such precision, timing, coordination and focus, while offering such stringent demands on flight crews and aircraft systems. Flight crews and airlines expect 100% success in such maneuvers while permitting neither tolerance for failure nor accident regardless of Probable Cause factors resulting from the gap in “Unusuality” factors.
Because of the increased use and reliance on automated flight control and navigation systems,[27] flight crews may possess a great ally in dealing with high stressors. Unusuality successfully most nights. But if the automation is not available due to an employment of a non-precision approach runway, lapse in their awareness of actual navigational positioning, or their positioning either laterally or vertically during an approach to instrument minimums, the level of Unusuality could exceed that crew’s abilities and prove hazardous and disastrous. An over reliance on systems that do the “flying for you” may result in degraded manual flight skills that may be needed to be maintained so as to detect the subtle changes in a/c tactile response because of accumulated icing on flight control systems or recover from unexpected windshear or wake turbulence.[28]
A pitot static system malfunctions may be incorrectly diagnosed when a well founded manual flying skill level might have reasonably detected the error and provided suitable systems knowledge and flying skills to correct the problem [29]. On 29 November 1963
Trans-Canada Air Lines Flight 831 a DC-8-54F, crashed at Sainte-Thérèse-de-Blainville, Canada. All 118 on board were killed; the cause was not determined, but pitot icing, vertical gyro failure, and pitch trim compensator problems were suspected. [30]
Negative stressors directly degrade the flight crew in the performance of their duties. With improved methods for identifying the potential of stressors overwhelming normal operations into a zone of Unusuality that may impact a flight, mitigation by the flight crew and dispatcher can be reasonably considered.
Stressors that combine to raise Unusuality include (partial list):
Fog/Low visibility Convective weather/TRW Compressed ATC vectoring
Non-precision approach Ignoring SOP’s Unfamiliar airport High terrain in A/P area Language difficulties Fatigue issues
Crew Coordination Errors Inside-Outside Manuever Performance MELs High intensity ops Low time experience Line training Ops
Night Operations Flight crew incompatibility Crew-Dispatcher disconnect
High frequency IMC ops Information “stovepipes” Automation Inattentiveness
Environmentals Vague limitations & guidelines Runway contamination
De-icing/anti-icing System complexity Uncontrolled Airports

Each of these stressors individually will not cause an aircraft accident, but the cumulative effect will result when two or more elements combine to surpass the crew’s abilities. This cumulative effect will have a “negative synergy” directly impacting and degrading the flight crew’s performance just when the operation may require crew precision and full operational optimization. Demanding operating requirements and diminished safety margins may limit alternative actions by the flight crew because of human or aircraft limitations.
While each “unusuality” stressor may not statistically cause an accident, if the flight crew is required to operate effectively while fatigued, execute a non-precision approach at night in marginal IMC conditions to an unfamiliar airfield, they may have a statistically reduced chance of success for completing the complicated maneuver. When optimal flight crew integration and performance is required for a successful completion, the stressors present may degrade the flight crew’s performance to the point failure .
For example, if given the same non-precision approach with slightly better weather, if the flight crew was experienced, well trained and rested, the chances of success would be greater, At what point in an operation is the safety margin impacted and degraded sufficiently resulting in an accident? Could awareness of causal factors be identified so as to better prepare a flight crew for the added hazard? Could flight crews and dispatchers be better trained at foreseeing such stressors?
Having just successfully completed Initial Operating Experience (IOE), that flight crew member must now operate optimally as a fully qualified and trained flight crew member. If that level of training proficiency cannot be achieved or maintained, the other crew member will be placed at a disadvantage that may not be fully recognized soon enough during the stressful and demanding final approach phase to an airport in marginal IMC conditions during a non-precision approach. Yet, all flight crews are trained and fully expected to successfully execute such an approach under any condition. There will be an imbalance in flight crew performance when the effects of the “unusuality” stressors combine to further degrade an already taxed flight crew.
Reviewing multiple aircraft accidents produces few unique Probable Causes. Can these Probable Causes be further reduced or eliminated with better training, more effective workforce integration, and improved knowledge sharing?
Consider the probable cause in a Controlled Flight Into Terrain accident such as Airbus A-300, UPS 1354 at Birmingham, AL, in August 2013.
The Probable Cause as stated in the NTSB AAR:
“Continuation of an unstabilized approach; failure to monitor aircraft’s altitude”.
The Contributing Causes included;
Failure to configure and verify the Flight Management Computer (FMC), Captain’s failure to communicate with the first officer about the FMC’s failure to capture the FMS constructed glideslope; flight crew’s expectation with regards to airport weather (above minimums), first officer’s failure to make callouts “minimums”, captain’s performance deficiencies, fatigue and distraction; and first officer’s fatigue.
The following “Unusuality” stressors were identified:
Night IMC Non-precision approach Low hours FO (403 hrs) Unstabilized approach Failure of SOP’s Fatigue
Dispatch disconnected Below minimums weather FMS operation not verified
Authority gradient Crew coordination Inside-Outside Maneuver Equipment not utilized Equipment complexity Inconsistent manuals
Marginal check-ride performance
Underlying the Probable Cause of this crash, these individual “unusuality” stressors probably would not result in a crash in themselves, but it is the authors’ submission that their cumulative effects directly contributed to the Probable Cause(s) thereby resulting in this crash.
- ) Night instrument conditions
- Only the non-precision LOC 18 instrument approach (ILS out of service for maintenance) was available. Less than Visual Meteriological Condition (VMC) existed. The reported visibility was less than 3 miles, broken or overcast ceilings less than 1,000 feet above ground level. Because the flight crew had received the airport report indicating that the ceiling and visibility were above the Localizer non-precision approach minimums, they believed that they would be able to successfully execute the approach and land. Either the company dispatcher or approach controller could have advised the crew that the most recent weather was now below non-precision minimums, but the crew was not aware of deteriorating weather conditions. If the Pilot Monitoring (PM), in this case the first officer had properly programed the FMC for the approach and then the Pilot Flying (PF) had executed the approach to minimums adhering to standard operating procedures, the crew would have then executed a missed approach when it did not acquire the runway at the approach minimums.
- The captain while flying the approach using the FMC observed the system NOT intercept the manually programmed glide path and had to insert his sink rate to catch up and capture the FMC glide path from above. He inserted a vertical sink rate of 1,500 feet per minute (FPM) which violated the SOP Stabilized Approach requirements of no more than 1,000 FPM when below 1,000’ agl.
- ) The first officer had limited Airbus experience.

- The first officer’s did not catch the captain’s error programming the FMC. When the captain continued the approach below Minimum Decent Altitude (MDA), the FO had already failed to call out “1,000 above (MDA)” and then “minimums”. This indicates a loss of special awareness on both the captain and FO as both were now trying to establish the aircraft on the desired The FO was not assertive enough as the approach deteriorated further. The FO questioned the captain’s intentions “Do you want to go around”? Instead of aiding him to make the decision to go around, she had asked him a question while he was conducting the approach, thereby further distracting him in his already stressed state.
- With less than 500 hours in the aircraft, she was still acquiring normal flying and crew skills and SOP interaction patterns. The FO, now as the PM would normally not need to direct a more proficient and experienced captain to do something that he did ask for or want. At some point, the approach was becoming more unstable to the point of being unsalvagable with a high decent rate and diminishing airspeed. Well outside of SOP’s (no more than 1,000 ft sink rate below 1,000 ft AGL; airspeed no slower than Reference speed (Vref)). Both excessive decent rate and airspeed below Referenced Speed (Vref) are two distinct callouts required of the pilot monitoring, but were both missed. Because both calls were missed, the effective backup of the PM provided to the PF were missed.
- The first officer’s attention was now mainly outside in an attempt to acquire the expected runway approach lights and the PAPI. If the FO had observed the Captain’s excessive decent rate and slow airspeed and then assertively called the captain on it, the captain may have then recognized his deteriorating and precarious position and executed a missed approach. By missing both the captain’s decent rate and slow airspeed, both crew members allowed the aircraft to be placed in an even more unstabilized and precarious position.
- ) Non-precision approaches are not overly demanding if practiced regularly. Due to the prevailing weather (wind) patterns, most airport approaches are constructed for the ILS, while in good weather conditions, many “visual” approaches are conducted.
- When well rehearsed and practiced, non-precision approaches demonstrate flight crew proficiency and coordination. When both crew members know and complete their SOP defined and required duties in this well rehearsed interaction, a demanding but not difficult approach while requiring attention, is not inherently dangerous. Both crew members need to have confidence in the other’s abilities and skill consistency, especially when conducting a non-precision approach.
- The Pilot Flying (PF) attention will be primarily inside on flight instruments, while the Pilot Monitoring (PM) will be backing up and verifying the PF’s actions. The PM’s attention will shift from mostly inside (backup of PF) to inside-outside to acquire the runway environment (approach lights, runway end identifier strobe lights, runway, etc.) while the aircraft descends towards minimums. Because this is mostly a PF controlled descent, the PF must integrate his actions and make considerably MORE flight management decisions (instrument course lineup, airspeed, descent rate, altitude until Minimum Decision Altitude (MDA) is reached; observing 1,000 feet and 100 feet above MDA (PM’s callout), approaching minimums, minimums, airspeed, decent rate, aircraft configurations, lineup to course (left or right of course) and checklist completion.

- Note, that when an aircraft is manually flown, for every PF corrective action to place the aircraft in the desired attitude (airspeed) and position (example: aircraft slightly slow, the PF would increase engine power and then when the desired speed is reached must now make a second correction so as to not get fast). If the autopilot is engaged, the auto-trim function will maintain aircraft stability (auto-trim pitch up or down). For every pilot flying correction, there is a required stabilizing second and third correction to maintain course lineup, airspeed and decent rate. PF must continually monitor-correct, monitor-correct, and monitor-correct to decrease aircraft displacements from the desired lineup, airspeed, and decent rate. When done correctly, this monitor-correct technique will result in decreasing oscillations positions. This aircraft-position monitoring is called “instrument scan” where information is visually processed, and then corrections and re-corrections are made.
- In an FMS enabled precision ILS coupled approach, the PF’s workload is significantly less and the aircraft’s stability is automatically maintained. Because of automation, immediate corrections to displacements are immediately corrected multiple times per second. Both pilots monitor and verify the FMS and autopilot systems.
- Cockpit workloads are significantly more demanding for a non-precision approach with increased workloads at lower altitudes closer to the ground where safety margins are more demanding and critical. The PM must carefully time-manage the duties (inside monitor-outside looking) and backup for the PF. This crew interaction, while executing and monitoring the progress of the approach is a well rehearsed choreography. If the PM spends too much time inside backing the PF, the runway environment will not be detected soon enough. If the PM spends a greater portion of time outside looking for the runway environment, PF deviations in course, altitude, airspeed, sink rate may go unobserved. Mutual confidence in the other’s flying skills and training is critical to execute this critical maneuvering successfully. Like playing the saxophone, it is easy to do poorly.
- As a Precision Approach Path Indicator (PAPI) system was available for an aid in landing on RW18 and if seen at approach MDA would have indicated the a/c transitioning from high glidepath, on glidepath, to below glidepath, why the PM detecting the runway environment and PAPI made no reference to the PF remains unclear.
- Ignoring Standard Operating Procedures (SOP’s).

- As Standard Operation Procedures are developed and updated, they provide a source document for operational standardization, training, and checking. SOP’s should match the realities of operations where you would not do something unless it was authorized. But, like speed limit signs on highways, many flight crews will test the boundaries, some partially, others fragrantly. Occasionally, a flight crew’s failure to comply with SOP’s can be evident in the AAR. Most SOP failures are caused by the flight crew trying to save or make up time on a flight. Some examples include: exceeding 250 kias below 10,000 feet; accepting a visual approach; maintaining higher speed during the approach; taking a closer but less suitable runway; continuing an approach when not stabilized below 1,000 ft AGL; accepting ATC’s direction to “(visually) follow traffic” for landing;
- ) Unstabilized Approach continued.
- SOP’s specify the criteria for a stabilized approach. Flight crews must adhere to those SOP’s and vigorously support their criteria in both word and practice. When ATC attempts to place the aircraft in a position that would infringe on those SOP’s, the flight crew should state that infringement and ask ATC if it was “essential” for safe operations? Examples of infringement: “Slam dunk” approaches”; high and close to airport; following too close an interval on a visual approach; vectors into weather on arrival route; not allowing a delay in the holding pattern for weather to clear; etc.
- Flight crews should freely accept “supporting input” from the other FC member when SPO’s are infringed (sink rate too high, approach airspeed outside of desired gates, off centerline on approach, off glideslope, not meeting non-precision approach gates, new influencing weather (tail wind, crosswind component, ground speed change, convective weather). The senior flight crew member should brief the other FC member to point out any observed unintentional SOP’s irregularities and do so without fear of retribution.
- ) Dispatch Disconnected.
- As the Dispatcher assumes equal responsibility for the flight (FAR xxx), the dispatcher should actively monitor that flight until its successful conclusion particularly if negative stressors exist and conditions warrant (weather changes, NOTAMs, weather near or below instrument approach minimums, potentially fatigued FC’s, etc.).
- The dispatcher has access to the destination’s airport or approach controller so as to acquire the most current information to assist the FC. This information can be readily passed to the FC to assist them.
- ) Flight Below Instrument Approach Minimums.
- Continued flight below the decision height or minimum decent altitude is counter to best practices, yet some FC’s continue such practice occasionally. Open or closed forums “Hangar talk” discussions among pilots concerning such practices should point out how precarious such maneuvers are and how such practices establish examples of negative learning patterns. The costs for such practices should diminish their occurrences.
- Some non-precision approaches require the FC to calculate a Visual Descent Point (VDP) after which a missed approach should be executed if the airport environment is clearly not established. F/C’s should freely discuss and clearly understand the importance and inherent dangers if the VDP is passed and a missed approach is not conducted in the misplaced hope of acquiring the airport at some later point.
- ) Flight Management System (FMS).
- Flight crews should use Flight Management Systems, GPS, etc as a tool to assist them and to decrease their en route workloads. These tools aid the FC, and do not take the place of the flight crew. Flight crews should be hone their flying skills as workloads permit. Basic special awareness is important to be maintained so as to detect a mis-programming of the FMS. The impact of operations with MEL out of service or diminished service availability items should be discussed as it relates to the expected flight conditions.
- ) Authority Gradient.
- Junior F/C members should consider how they will effectively interact with the senior FC member and the best practices for communicating. While deference to seniority might be appreciated, the junior member should be encouraged to actively participate in all duties expected from that position including assisting the senior FC member. Full communications and the free flowing of information to add to the safe completion of the flight should be emphasized and encouraged. The F/C should be sensitive to effective communication techniques in order to support full cockpit resource management.
- When new crew members first begin flying together, the Captain should discuss the effective communications, overall crew responsibilities and best practices for cooperation. It should be realized that some senor staff/check pilots may be at a disadvantage in trying to maintain required currency because of their staff jobs. All flight deck members should be encouraged to exchange information related to SOP irregularities. While the captain retains absolute authority for the flight, no one is served if an observed SOP error jeopardizes the safety of the flight. should be pointed out and discussed as needed, regardless of rank and seniority.
- Recent airline mergers from one-time competitors places added pressure on the effective flight deck communications of now merged flight crews. Company differences and union affiliations need to be minimized, and the preservation of professional safety standards need to be enforced. This will be difficult to achieve in the confines of the closed door flight deck but essential for safety.
- ) Crew Coordination. Coordinating flight deck efforts while at altitude while the aircraft is on autopilot are of limited intensity and require only routine coordination. One member flies the aircraft while the other performs navigation and communications functions. Both members back each other up. Routinely, these duties are alternated on each leg of the flight. As the flight intensity and flight deck workload increase during the arrival, approach and landing phases, clear duties and responsibilities as defined in the SOP’s need to be completed with no ambiguities as to whom will be doing what functions and when. While SOP’s define the roles of each pilot, AAR’s indicate repeated errors in execution or lapses in performing those duties remain present.
- ) Inside-outside duties on approach. Although flight deck duties during the terminal phase are sufficiently defined, the allowable safety margins are critical given the speed of the aircraft, energy-momentum levels (weight of a/c, speed, decent rate) progressing flight path, and closing proximity to the ground.
- Although flight deck duties during the terminal phase are sufficiently defined, the safety margins are critical given the speed of the aircraft, energy-momentum levels (weight of a/c, speed, decent rate) progressing flight path, and closing proximity to the ground.
- The duties of the pilot flying (PF) when completing a terminal phase of flight while in IMC conditions test the skills and the training of both FC members. The FC’s workload with the autopilot engaged significantly reduces monitoring and PF inputs (observe and verify with no real-time critical action requirement to “do” until either the airport environment is established or the a/c nears approach minimums). If a non-precision approach is being conducted, FC workloads increase significantly as the a/c is flown to a critical position in airspace in relation to the runway (altitude and lineup). The PM must monitor the a/c’s altitude as it approaches the MDA making the appropriate altitude callouts (1,000 above, 400/500 above, minimums) to the PF while the monitoring the a/c’s airspeed and decent rate.
- The PM may have only a few final seconds to monitor the PF’s aircraft positioning and a/c’s momentum, while also trying to sufficiently detect the runway environment. Once the runway environment is detected, suitably recognized (left or right of runway centerline and positioning on a visual glide slope (VASI/PAPI), this must be quickly and accurately conveyed to the PF. The PF must now leave the inside instrument scan to now acquire the runway environment, VASI/PAPI glideslope positioning, and then transition the a/c to land; ALL within the safe parameters of kinetic energy and a/c trajectory., When landing is accomplished, determine if the touchdown point is sufficient to allow the aircraft to safely stop within the remaining runway. The PF must manage the a/c’s trajectory and deceleration to a safe taxi speed is attained given the conditions of the runway (wet, standing water, braking action, packed snow, grooved/non-grooved, wind velocity and direction, and the a/c’s hydroplaning characteristics).
- ) Equipment not utilized
- ) Equipment Complexity, Inconsistent Manuals




From Wikipedia on line
http://en.wikipedia.org/wiki/UPS_Airlines_Flight_1354UPS
- “Airlines Flight 1354 was a scheduled cargo flight from Louisville International Airport to Birmingham–Shuttlesworth International Airport. On August 14, 2013, the aircraft flying this route, a UPS Airlines Airbus A300-600F, crashed and burst into flames short of the runway on approach to Birmingham–Shuttlesworth International Airport in the US state of Alabama. Both pilots were pronounced dead at the scene of the crash. They were the only people aboard the aircraft.
- Aircraft: The aircraft involved in the accident was an Airbus A300F4-622R, registered as N155UP. It was built in 2003; UPS took delivery of it in February 2004. It was powered by Pratt & Whitney PW4000 At the time of the accident, it had accumulated approximately 11,000 flight hours in 6,800 flight cycles (takeoff-and-landing sets).


Crash: The aircraft crashed at about 04:47 local time (CDT, 09:47 UTC) on approach to runway 18 at Birmingham–Shuttlesworth International Airport. It clipped trees and struck ground three times uphill. The fuselage broke apart, with the nose coming to rest about 200 yards (180 m) away from the initial point of impact, and the rest of it about 80 yards (70 m) further down towards the runway and about 1 kilometer (0.6 mi) from its edge and catching fire.
Investigation: The National Transportation Safety Board (NTSB) launched an investigation and sent a 26-member “go team” to the crash site to “collect perishable evidence”. At a press conference held later on the same day, the NTSB said they had been unable to recover the cockpit voice recorder and the flight data recorder as the tail section (where the recorders are housed) was still on fire. Both recorders were recovered on the following day, and were sent for analysis.
On August 16, 2013, at their third media briefing, the NTSB reported that the crew received two GPWS alerts “sink rate!” (that they were descending too quickly) 16 seconds before the end of the recording. Three seconds later, one of the pilots commented that they had the runway in sight. Nine seconds before the end of the recording, impact sounds were audible. The crew had briefed the approach to runway 18 and were cleared to land by air traffic control two minutes prior to the end of the recording. The captain was the pilot flying, and the autopilot was engaged at the time of the accident.
To represent the country of manufacture, the French aviation accident investigation agency BEA, assisted by Airbus technical advisors, participated in the investigation. Members of the FBI Evidence Response Team also assisted the NTSB. The NTSB stated in late August that no mechanical anomalies had been uncovered to that point, but that the complete investigation would take several months.
On February 20, 2014, the NTSB held a public hearing in connection with its investigation. At that hearing, excerpts from the cockpit voice recorder were presented, in which both pilot and co-pilot discussed their lack of sufficient sleep prior to the flight.
In 2014, the Independent Pilots Association filed suit against the FAA to end the cargo airplane exemption from the flight crew minimum rest requirements.
On September 9, 2014 the National Transportation Safety Board announced that it had determined the probable cause of the accident was that the aircrew had continued an unstabilized approach into Birmingham-Shuttlesworth International Airport during which they failed to monitor their altitude and thus inadvertently descended below the minimum descent altitude when the runway was not yet in sight resulting in controlled flight into terrain (CFIT) approximately 3,300 feet short of the runway threshold. The NTSB also found contributing factors to the accident included: 1) the flight crew’s failure to properly configure and verify the flight management computer for the profile approach; 2) the captain’s failure to communicate his intentions to the first officer once it became apparent the vertical profile was not captured; 3) the flight crew’s expectation that they would break out of the clouds at 1,000 feet above ground level due to incomplete weather information; 4) the first officer’s failure to make the required minimums callouts; 5) the captain’s performance deficiencies likely due to factors including, but not limited to, fatigue, distraction, or confusion, consistent with performance deficiencies exhibited during training, and; 6) the first officer’s fatigue due to acute sleep loss resulting from her ineffective off-duty time management and circadian factor.” Note: Wikipedia footnotes omitted, but are in the referenced original text.
However, let’s take another look at the mishap of UPS 1354.
We will list the Negative Stressors, when the stressors were known and by whom they were known:
- Night flight ops; scheduled; all knew including tower ATC operators and airfield maint.
- High terrain in approach corridor; charted; all knew
- Crew fatigue due to night scheduling; scheduled; well known industry fatigue issue
- Additional fatigue vector-crew was not feeling rested enough to perform well; crew discussed in flight; crew knew
- Weather reported above mins at 1000 feet, actually 200-300, below mins, misleading them to believe they were 1000′ agl when they broke out of overcast.
- Non precision approach. Published, but crew might have been expecting the ILS. The non precision approach was known by all well before the mishap, but as the name implies, it lacks the glide slope precision information that is critically important in the Category two and three ILS certification for which this plane and this crew were qualified. The Cat II/III runway was not available due to an electrician changing light bulbs on that runway. It was never determined if this was scheduled or non-scheduled maintenance, although a notice to airmen was published. It should be noted that the arrival times for UPS 1354 are also published at least two months in advance and therefore well known to the local ATC office and airfield engineering.
- Ineffective CRM, PF was doing it on his own putting in high sink rate to get down to MDA after FMC didn’t engage. Known after from CVR
- FC violated SOP for a stabilized approach, over 1,000 fpm decent under 1,000 ft agl. CVR
- PM didn’t call out callouts CVR
- PM was outside (looking for lights) and inside (trying to backup PF and make callouts) CVR
- Pilot-Dispatcher disconnect, dispatcher didn’t give help with weather. While the weather was called as 1000 feet above field elevation, in the RW 18 corridor, it was between 200 and 350 feet above the ground level.
- Airport did not do a decent threat analysis on light maintenance on ILS vs. crew coming in in bad weather for a non-precision from scheduling information known 2 months in advance.
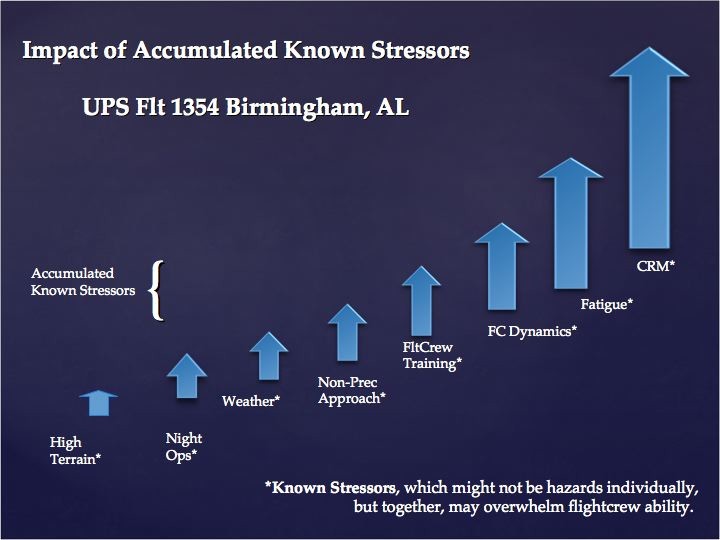
Figure 1. Impact of Accumulated Known Stressors, UPS 1354, is a pictorial depiction of this idea, remembering that stressors may not individually be considered hazards to flight in and of themselves. However, in the accumulation of stressors, we may have found that the accumulation itself may be a new unrecognized hazard, the one ultimately overwhelming the crew.
What do you think?
Could it be that by looking at the sum total of the negative stressors, we may find that real hazard that led to the UPS 1354 mishap? In so doing, could we find a pattern of crew overload, an overwhelming of the crew ability at any one point in time? Could this be the area that flight safety managers need to look at next to bring the commercial airline mishap rate closer towards zero?
Collectivity of Mishap Causes as a separate issue.
In our study of multiple commercial aviation mishaps[31], the mishap investigation boards publish what appears to be a listing of probably and contributing causes, each listed singularly. The purpose of listing the causes singularly is so that the authority, agency or organization accountable for making changes to equipment, procedures for interacting with the flight environment and standard operating procedures that humans use, can address each cause with an action to prevent the same mishap from occurring again.
However, we noticed that in each boards mishap investigation report, that there was also a collectivity of causes, a set of cascading facts, an accumulation of events, that could be derived by looking at reporting patterns of the investigators. Further, as commercial airline pilots we recognized that in many mishaps, the collectivity of mishap causes, in and of itself, in addition to singular and individual causes, seems to overwhelm the crew. If they did not make the right decision immediately in reaction to the events, subsequent events began to pile up, accumulate and eventually overwhelm the crews’ ability to react to successfully bring the aircraft to a safe landing.
In the USAir 1549 Airbus landing on the Hudson River, the crew was faced with a set of negative stressors, but through superior crew ability landed the aircraft in the water allowing the survival of every person on the flight.[32]
In the United 232 DC10 landing in Sioux City, Iowa,[33] and the Ethiopian Airlines 962 B767 mishap in Tanzania[34], the crew exhibited superior ability in the face of overwhelming negative stressors, allowing many onboard to survive what could have been totally fatal mishaps. The level of Unusuality reached a very small positive value in the final few seconds of each flight causing the landings to be high speed and resulting in airframe break up. However, the crews stayed ahead of the negative stressors right until the last moments and as a result, the level of Unusuality was very small.

In other mishaps, the crews were certified, fully trained and qualified according to the standards of the day, yet the accumulation of negative stressors in and of itself, and not just each individual cause, may have overwhelmed the crews’ ability to react to successfully bring the aircraft to a safe landing. One popular view is that when viewed individually, each negative stressor is manageable and therefore the crews could have saved many of these flights. However, this is not our argument, since the authors looked at the mishap reports from the viewpoint of collectivity of mishap causes. From this view, a straw can break a camel’s back. [35]
In Swiss Air 111[36] off Nova Scotia, in Singapore 006[37] at Taipei, in Southwest 1248[38] at Midway, Chicago, in Alaska Airlines 261[39] and in American Eagle 4184[40] the crews were faced with a set of accumulative negative stressors that occurred simultaneously or in very quick succession and appear to have overwhelmed the crews’ ability to react successfully.
In Swiss Air 111, incorrect design, engineering, documentation and procedures were occurring, as an electrical malfunction became a source for fire. Negative stressors exceeded the crew ability and created a positive level of Unusuality.
In Singapore 006, a swirling typhoon rainstorm blanked out visibility. This prohibited the ATC tower controller from observing that of the two sets of operating green taxiway lead-in lights were lit, one to the correct runway and one to a runway closed for construction and occupied by heavy equipment. The construction was also invisible from the cockpit due to rain. Singapore 006 crew had inadvertently followed the lights to the closed runway and begun takeoff. The negative stressors accumulated past the crew’s and ATC controller’s ability at that time and created a positive level of Unusuality.
In Southwest 1248, the crew was faced with a runway in snow with a tailwind and lacked familiarity with some aircraft systems. Stopping distance calculation procedures used available thrust reverse, which if unused or unavailable could prevent stopping in slippery conditions. In all, the tailwind, snow and questionable calculations, along with the misuse of thrust reversers accumulated negative stressors greater than the crew ability at the time to react and resulted in a positive level of Unusuality,
In Alaska 261, the crew, by attempting to discern a way to reestablish pitch control after the pitch control systems malfunctioned, and unaware that their actions added to the accumulating negative stressors, which included incorrect maintenance procedures, eventually became overwhelmed when the damaged pitch control system totally failed causing a subsequent unrecoverable aerodynamic longitudinal stability failure. So there was both a stability failure and a control failure occurring at the same time, as the failed jackscrew that adjusted pitch control, also held the horizontal stabilizer in position.
In American Eagle 4184, the crew was placed in an area of icing to hold. The airframe icing buildup that was investigated was downstream of deicing systems but upstream of aileron controls. The weather was IMC with icing, it was night time reducing visibility, no engineering or test data documentation was available for long term in-flight icing exposure, no limit-time existed in FAA ATC regulations for holding in icing conditions. Meteorological ability to discern levels of icing between light, moderate and heavy were dependent upon a calculative synthetic estimate of flight level precipitation and freezing temperatures and therefore only advisory in nature to ground stations such as ATC and dispatch. The negative factors, all known about ahead of time, accumulated during the flight of AE4184 and overwhelmed this crew’s ability to react in a manner to successfully control and land the aircraft. Unusuality in this case existed because the sum of the negative stressors exceeded the crew ability.
In Executive Airline (doing business as American Eagle) 5401 mishap[41] in San Juan, many crew-training issues came to light, but training is based on procedures. The board determined that bounced landing procedures and thus training was insufficient to address the circumstances when an ATR 72 landing bounce occurs. The crew ability was a vector of a lower magnitude than the vectors of the negative stressors on this flight. While the flight was not a training flight, the pilot flying has recently completed IOE training, but that training did not include bounced landing procedures. This is an example where the crew ability was low and the negative stressor vector exceeded the ability vector resulting in positive Unusuality.
The mishaps were the result of an accumulation of many negative stressors, negative factors whose vectors collectively far exceeded the crew ability at that time to successfully land the aircraft. The collectivity of the mishap causes and not just each cause individually may be an important unaddressed factor in commercial aviation mishaps.
Recognizing Known or Knowable Negative Stressors
Each of the negative stressors was either a known fact before the mishap or it was a knowable fact before the mishap. In each of the mishap board investigation reports, each probable cause and contributing cause listed for these mishaps was either known or knowable before the mishap.[42] [43] [44]
Some may argue against this known or knowable claim concerning the ice horn build up discovered in testing after the AE4184 mishap, [45] [46] citing the tests as the source of knowledge and the date of the testing subsequent to the mishap.
Quite to the contrary however is the fact that super-cooled particle physics is not a new subject and has been known thermodynamically for a very long time. [47] Noted physics writers Halliday and Resnick describe super cooled liquid physics in their text earlier published in 1962. Super cooled liquids changing phase into solids without an intervening loss of heat energy normally associated with phase change from liquid into solid is described. The danger of flight into rain, water that has cooled below the normal freezing temperature is that upon phase change, the volume of ice created by the freezing water in much higher than the build up of ice that has already formed in the atmosphere, since ice by volume is greater than water by volume at the same weight. [48]
While testing may have employed ATR 72 aircraft parts to determine the exact nature of the icing build up, the physics of massive ice build up due to impact with super cooled liquids was a known fact well before the mishap and thus was a knowable negative stressor in existence before the mishap occurred. Would the variation of different crew members on that flight changed the rapid build up of super cooled water into ice on the ATR 72 airframe the night of the mishap? The way to prevent the build up of super cooled water into ice would have been to avoid flight into that area of precipitation. Since the crew was directed into that area by ATC, should does ATC have a responsibility to know knowable facts, such as where in the control area are conditions for super cooled rain, known as freezing rain likely to exist. Could the airline dispatcher, who also had access to and knowledge of real-time meteorological data adjusted operating procedures such as flight plan to avoid freezing rain areas?
The freezing rain occurrence and consequence to flight safety was known and knowable before the mishap.
In Asiana 210 at San Francisco, in Korean Air 801 at Guam and in UPS 1354 at Birmingham, for a variety of reasons, the precision ILS equipment was withdrawn from service and unavailable to the crewmembers. Crew members were operating very large aircraft filled with passengers and had multiple human factors issues such as language spoken not being English as a first language, fatigue due to long operating periods, in two cases at night in areas of terrain above the field elevation. In all three cases, the aircraft and the airfield were capable of very precise and sophisticated automated landings. The automated landing technologies for plane and airfield had been developed to improve commercial flight safety. Locally at those airfields, a decision was made to withdraw that equipment from service. No longer would this technology for safe flight be used. Instead, the ATC manager substituted much older and less effective airfield avionic equipment, lacking electronic glideslope information critically required to allow the crew to couple the aircraft autopilot systems to the airfield equipment. This was initiated with just the minimum of notice to airmen. The airline choose to dispatch these flights knowing that the latest technology was out of service and the airfield ATC managers choose to continue commercial flight operations knowing that the latest technology had been withdrawn from service. Because these were long flights and conducted during circadian low cycle times, crew fatigue is a negative stressor, whether or not recognized by the investigating board. [49] [50] [51] [52]
Operating demands in these circumstances increased very significantly while the negative stressor vectors of fatigue and other factors affected the crew ability. In these three cases, the negative stressor vectors surpassed crew ability and the positive vector of Unusuality occurred.
In the KLM 4805 and PanAm 1736 twin B747 disaster at Tenerife, negative stressors once again began to add up.[53] Weather visibility prevented visual ATC confirmation of aircraft movement around the airfield and prevented aircrew in each aircraft from seeing other aircraft moving about the airfield. Earlier diversions of large aircraft had overburdened the parking and taxiway areas of the airport. Since many flights were long distance operations, crew duty day and fatigue issues added negative stressors. English spoken as a second language was a human factor negative stressor vector. In addition to the overburdened surface movement area, the radio frequencies available for usage were overburdened, resulting in more than one aircraft transmission occurring simultaneously, this causing some aircraft receivers to not process the multiple transmissions clearly, this resulting in miscommunications and missed communications. Once again, the mishap boards investigating this enormous disaster cite many probable causes and many contributing causes.[54]
Our study though looks at the cumulative effect of all of the negative stressors and compares that to the crew ability available at that time. For ATC and the crew of KLM 4805, the level of negative stressors surpassed their abilities and a positive value for Unusuality occurred. However, each investigation found factual evidence that was known or knowable at the time of the mishap. For example, the crew of KLM 4805 was able to hear the multiple radio transmissions between ATC tower and other aircraft moving on the airfield under tower control. Even though there is not direct procedural requirement for any crew to monitor communications with other flight crews, the communications between tower and Pan Am 1736 were received by KLM 4805 and were knowable. In addition, both tower and Pan Am 1736 transmitted information that contained location information on where Pan Am 1736 was, and the radio traffic clearly stated the location of Pan Am 1736 as being taxiing on the same runway that KLM 4805 was holding in position for departure[55]. The mishap investigations did not discover any fact that was not already known or knowable to the crew of KLM 4805. The tower radio transcript and the cockpit voice recorder transcript for Pan Am 1736 [56] clearly show that the crew of Pan Am 1736 knew that KLM 4805 was anxious to depart and may have already started take off roll without explicit tower authorization. The level of negative stressors in this case impacted the crew of Pan Am who were aware of ATC communication irregularities with KLM 4805 and despite their best efforts and abilities, were overcome by the compilation of negative stressor vectors and fell victim to a positive value of Unusuality.
At Buffalo, many negative stressor vectors added up to a value greater than Colgan Air 3407 crew’s ability. CRM and crew aircraft handling training were very weak vectors. Nighttime ops and crew fatigue were negative crew ability vectors. Unusuality became a positive value due to very low crew ability values. [57]
By contrast, the crew of American 1420 at Little Rock was well trained and experienced in procedures.[58] However, the demands on the crew grew well above normal ops when they arrived at the scheduled airfield in the midst of severe thunderstorms, during night operations, requested and were cleared to land on a rain contaminated runway with a very strong crosswind, no headwind and possibly a slight tailwind. While the crew delayed opening thrust reversers and did not deploy wing spoilers in either auto or manual mode, other negative stressors may have added vectors in the wrong direction.
For example, when the American Airlines dispatcher looked at the local radar remotely at the airline hub in DFW, was the dispatcher seeing calculated rain decibel return or wind field data? Again, in reviewing the NTSB AAR, the causes related to the aircraft loosing directional control and being unable to stop were related to the wind field on the runway at the time. While rain contaminated the crowned and grooved runway, reducing runway tire friction, was not the wind the actual physical force the moved the aircraft? From Newtonian physics,[59] forces can only be made by bodies and in this case, the body was the wind field of moving air. It was not the rain that moved the aircraft but the wind. Yet, the dispatcher was advising the flight crew based on data of the rain. The windfield data was loosely available to the dispatcher who could have calculated a wind field by comparing observed surface magnetic winds and 3000 foot true forecast winds, as well as charting observed surface wind changes being reported regularly. But instead, the dispatcher used reported radar rain data to advise the crew on a safe course of action. The crew could well have made the decision to hold or divert to a clear airport near by, citing negative stressor vectors as exceeding their abilities to land successfully at that time. However, they did not self diagnose the growing positive Unusuality.
Why? Did this airline or any airline have a self diagnosis procedure whereby flight crew could determine that the level of negative stressor vectors had exceeded their abilities at that time and they needed to pursue an alternate course of action, rather than allow Unusuality to affect their safety and the successful landing of their aircraft.

What would a Recognition Metric for Unusuality look like? If a recognition metric could be developed, could some procedural adjustment method be developed to intervene quickly to prevent a commercial aviation mishap?
A recognition metric for Unusuality would have to take into account several elements that have been discussed above:
- Collectivity of Causes as a separate issue:
The cumulative affect of many multiple probable causes and contributory causes identified in so many of the commercial mishap in the Williams and Miller Study of Commercial Aviation Mishaps Causes informs us that the goal of a recognition metric is to look for things that affect the people involved, the equipment involved and the flight environment. A working metric has to be looking at all three areas for hazards that are occurring at the present time and thus have been occur, at least since the recent past. The metric must be able to measure all of these hazards in some quantitative fashion, even if that methodology estimates the values of the hazards or negative stressors.
- The metric must be able to recognize negative stressors as vectors, that is, a value with both size and direction. It must be able to recognize that which is working against the crew and by how much. It should be remembered that negative stressors were in existence at the time of the mishap, were either known or were knowable facts, according to the NTSB and other boards who were able to find them as existing facts at the time of the mishap, weeks and months after the mishap.
- The metric must be able to identify whether the crew ability is 100% normal according to the standards for that airline, or whether the crew ability is diminished by human factors such as normal fatigue, or whether the crew ability is affected by strong, normal or weak levels of training as defined by the standards of that airline. The metric must be able to assign a quantitative number to represent the level of crew ability, perhaps in terms of 100% or some other value that is consistently applied by metric to all crewmembers at that airline.
- The metric should be able to classify a particular operation as normal for that airline, easy or perhaps more difficult than normally encountered. Again, a value system using percent as determined by that airline would be most applicable and useful.
- The metric must next be able to quantitatively compare the level of negative stressors as they are known or should be known to be occurring and affecting a particular flight, with the crew ability at that time for that flight. As long as the crew ability remains greater than the accumulative vector level of negative stressors, then the operation can continue using normal SOP. If training is effective and applicable to line operations, this case should be the predominate condition day to day.
6, However, in the few and rare cases when the crew, the dispatcher, the chief pilot or other authority determines that the negative stressor vectors are at a value that begins to exceed the current crew ability value, then the metric must be able to identify that a positive level of Unusuality is occurring. This means that hazardous conditions are occurring during this flight operation. This method differs somewhat to other quality assurance and risk assessment systems because the values being compared normally fluctuate throughout the day due to diurnal and nocturnal fatigue and by so many other factors that could increase or decrease both the value for crew ability and for negative stressors. It is a value dependent on comparing a series of variables with each other and understanding that value as acceptably normal or unacceptably unusual, possessing Unusuality.
- The pay-off however for this Unusuality Recognition Metric comes when the local flight authority, the team of crew and dispatcher or even the crew individually determines that there is a reason to make an adjustment to operating procedures that will bring the level of Unusuality back to zero or a non-positive value and thus prevent a mishap from ever occurring.
Of course, everyone would expect a standard formulation at this point to take home and plug-in to their flight operation. However, since safety at each airline is the result of effective locally applied programs to identify hazards and take quick action to eliminate them, the actual metric will have to be locally developed in order for it to be effective at each airline. There is no standard formulation, but there is an example below of how to create a metric for your airline.
The most important thing to remember is that negative stressor vectors are cumulative in nature and therefore, in order for the metric to work, it must measure negative stressor vectors that affect people, equipment and the environment.
Example Recognition Metric for Unusuality.
Here is an example of how a Recognition Metric for Unusuality could be created and applied in the case of the Air France 447 mishap that occurred off Brasil in the Atlantic Ocean area known as the inter-tropical convergence zone.
- What were some of the collective causes listed in the mishap report?
1.1 The environment: The report listed that weather in the inter-tropical convergence zone often contained very large areas of convective activity, both in terms of heights of clouds reaching 50,000 to 60,000 feet and areas of clouds with diameters in excess of 50 miles and in some cases much longer. This is a known negative stressor because the manufacturer, the regulator and the airline procedurally recommend avoiding thunderstorm activity.
But at the airline dispatch office, where real-time satellite photos were regularly on display, and at this time an area of thunderstorms reaching heights in excess of 50.000 feet stretching over a diameter of 70 miles along the planned and known flown flight path of AF 447, no communications rerouting the flight around the area of severe weather were calculated, communicated to the flight or investigated by the dispatch office with the ATC agency controlling that airspace. Add the negative stressor of night operations, where in the crew could not visually pick their way through an area of storms or visually recognize that there was no viable path other than to circumnavigate the area of convective weather.
Flight path deviations in oceanic zones are procedurally acceptable as a normal procedure coordinated between the controlling agency, the crew and the dispatch office.
1.2 Equipment: The Airbus 330 was a very solidly built transport aircraft, capable of withstanding g-forces, icing, wind gusts, lightning strikes, small hail and other hazards associated with inadvertent flight through thunderstorms. However, intentional flight through an area of 50,000 foot tall thunderstorms 70 miles wide, a transit which would last about 15 minutes at a cruise speed of 450 knots is not recommended because hail can reach size and hardness significantly damage aircraft leading edges, antennae, wind screens and engine fan and compressor blades. In addition, there was a known problem with the pitot static system installed on the aircraft, a problem of it malfunctioning in frozen precipitation. AF 447 was filed to fly at flight levels where any precipitation would be frozen precipitation. Losses of the inputs from the pitot system were known to cause considerable disruption to the computer-based management of flight on the AB 330. This was a known problem as loss of the pitot system on any transport aircraft is a considerable in-flight equipment problem.
1.3 People: The crew was well trained by Air France standards. The dispatcher was well trained by Air France standards. However, the captain left his station to two qualified crewmembers before the flight entered the inter tropical convergence zone. Since the zone was known to possess the potential for massive thunderstorms, perhaps it would have been a good idea to remain on the flight deck while the flight transited the zone. The other crewmembers appeared to be trained to respond to various warning and caution systems that began to go off, however they did not appear to be well trained in the procedure for loss of flight instruments. They also kept the aircraft nose raised during the stalled condition, which indicates that their aircraft handling training for such things as aerodynamic stalls was very weak. Lastly, the dispatcher showed little concern nor initiative to improve the safety of the flight by taking some actions to advise the crew of the hazardous weather ahead nor actions on how to avoid it. Was the dispatcher thinking of the welfare of the hundreds of passengers and crewmembers onboard AF447? Even if the flight made a successful transit of the severe convective weather area, the ride would have been very rough, uncomfortable at best, but also very hazardous to people not buckled in firmly with seat belts at worst.
- The negative stressors as vectors: When taken collectively, the known negative stressors in the flight of AF 447 added to a very big quantitative number. In addition, every negative stressor was known or was knowable ahead of time. The BEA report identified causes that were all known or knowable at the time of the mishap, thus these were facts existing at the time of the mishap and thus existing before the mishap occurred.
- The crew metric could be considered 100% trained and ready by the Air France standards. Possibly fatigue was affecting the captain, who self diagnosed and chose to take a nap after the aircraft was established on its oceanic track. Since there was a question about the crews aircraft handling ability, it would be fair to set he crew ability at perhaps 90% instead of 100%.
- The airline operation challenge for AF 447 could be considered normal, yet any transoceanic long-range intercontinental flight through the intertropical convergence zone is a level above the challenge of an intercity continental flight. The qualifications for this flight require extra procedures training and three crewmembers were assigned because of the long duty day. If a normal intercity flight were to be at a 20% level challenge for Air France, this flight would easily be considered twice that at the 40% challenging level.
- The comparison between the negative stressors, the operational challenge and the crew ability. Since the crew was totally qualified to operate this flight successfully and other crews similarly qualified had successfully operated this flight many times, it can quantitatively be stated that the crew ability was in excess of 40% and appeared to be at about 90 % from number three above.
However, when the collective negative stressors are added together as vectors and compared with the crew ability, it appears that the collective negative stressor exceeded the crew’s ability to successfully complete the flight. Does this mean that negative stressor for which they were ill prepared to handle overwhelmed the crew? Perhaps the crew ability should be moved lower to 80% or 70 %?
Does it mean that the collective negative stressors were so great that they overwhelmed the crew whether they were at 70, 80 or 90%? Did Unusuality occur, in that the value of the comparison between negative stressors and crew ability was positive and sizable? Was the crew not sufficiently trained or was the crew overwhelmed by Unusuality?
- Did the pitot system malfunction, the entry into a massive area of thunderstorms, the failure of the dispatcher to assist the flight, the absence of the captain initially from the flight deck, the crew’s poor aircraft handling ability collectively combine to overwhelm the crew’s lowered ability to successfully complete the flight operation?
- If the Recognition Metric for Unusuality has been successfully developed in steps 1-6, it is clear that each fact discovered by BEA was a fact and thus discoverable before the mishap occurred.
If Unusuality is a recognizable and measurable comparison between known or knowable facts before a mishap occurs, an adjustment of operating procedures could be made to avoid mishap’s occurrence even before it occurred.
One example would be for the airline to require the dispatcher to adjust filed flight paths for flights transiting the intertropical convergence zone when convective weather blocks their filed route. Another example would be for the regulator to require more immediate responses to known equipment hazards such as pitot systems known to fail in icing conditions. Another example would be for the airline to tailor their minimum equipment list or MEL for equipment needed on a particular type of flight such as a transoceanic flight through the intertropical convergence zone.
Another example would be for the airline to adjust procedures to require the captain’s presence during transit of forecast or known severe weather areas. In addition, there appears to be a need to improve aircraft handling training at this airline to include stall training and flight with inoperative flight instruments.
Conclusion:
IN CONCLUSION, there are three things to keep in mind.
1. This is one of our most innovative projects ever. Why? Here is why. Past mishap prevention procedures focused on hazard elimination. Hazard elimination works well and has helped us move forward up to this point. We continue to espouse hazard elimination as an important safety strategy.
But, we have found another “non-hazard” hazard lurking in plain sight. It is the overwhelming of flight crew members by negative stressors! Each negative stressor might not necessarily be classified as a hazard to flight by the current risk analysis methods used by most airlines.
However, when negative stressors are heaped together, they can build to the “tipping point.[1]” In remembering the book, “The Tipping Point: How Little Things Can Make a Big Difference (2000), by Malcolm Gladwell[2] negative stressors can combine to overwhelm crew members. It is very much like the story about “the straw that broke the camel’s back.” It wasn’t one straw or another that was the problem. Straw isn’t a problem. Negative stressors might not necessarily be considered hazards. It was when too many straws were placed on a perfectly good camel, the camel was just overwhelmed his ability to carry it all and collapsed.
It is the same way with flight crew. One day everything is fine, the flight is a success and they perform well. The next day so many things happen at once, all needing an immediate or relatively rapid response and the crew is overwhelmed and fail. This is what happened for example to AF 447, UPS 1354, KLM in Teneriffe, Swiss 111.
All of these crew members were successful and capable. But one day too much was served on their plate and they choked on it all. If you listen to Captain Sullenberger’s voice from the ATC broadcast tapes[3] and cockpit voice recorder, you can hear a guy speeding up his talking to two or three times his normal word per minute rate. He is not excited in tone, but he certainly is using his increased word count to communicate, giving him and his copilot time to set up and talk over options. He does not allow Laguardia Departure ATC to draw him into a prolonged discussion of what are now becoming irrelevant options. He does not issue a mayday call nor does he squawk mayday with his transponder. He knows now that no one can help him, he needs to do what needs to be done. He becomes his own rescuer. Once he landed safely, he said, “then we all needed to be rescued.”[4]
What is also notable to me is that ATC is baffled and eventually drops out of the conversation almost dumbfounded. But another voice on the frequency states, “I think he said that he is landing in the Hudson.” I believe that the comments are from the flight crew of another flight airborne on the same frequency, who grasp immediately Sully’s game plan and attempt to translate it to Laguardia Departure. [5]
So that is the first important insight. The crew one day is operating fine and the next day crash. Same crew, same plane, same operation. If a tipping point of negative stressors is reached or exceeded, the phenomena of Unusuality appears and can hazard safe commercial flight.
2. Second, each of the NTSB reports we reviewed in our study had one very important and common element in them: they all list somewhere in the report, numerous probable causes and contributing causes. Some reports listed between ten and twenty things that went wrong. Yes, the mishap board reports cite probable and contributing causes numbering often in the double digits!
What does that mean to us? For one thing, the crews of the mishap planes were having to deal not with just one hazard, one thing wrong , one negative stressor. No indeed. They were having to deal with ten to twenty things wrong and deal with them all at the exact same time. Isn’t that really what each of these NTSB and other board investigations state, whether they do so knowingly or unknowingly, when they issue their lists of probable and contributing causes? Yes? No? If not, how else could the causes be related to the mishap?
Each of these reports, in some cases ten to twenty probable and contributory causes, if they are indeed valid as causes, as the mishap board have stated they believe them to be the case, then each of these causes represents a problem, a hazard or a negative stressor that the crew was facing and to which they had to respond at the time of the mishap occurrence.
If indeed these after accident report are correct, and we have no reason to argue that they are not correct, then what the boards are stating is this: numerous things, in some cases, ten to twenty things went wrong at about the same time, that is, the time of the mishap, that the crew had to confront. The CVR and the DFDR, and the tower tapes and all the other factual evidence in all the reports, document a strangely similar set of events in each mishap. It is this: the crew members were faced with an large simultaneous set of issues that wound up overwhelming their ability to cope. It is that simple. The level of negative stressors exceeded their ability at that time. So to understand this, you have to understand that there are two variables. One is the level of negative stressors and the second is the ability of the crew at any given point in time. This can and does vary up and down. In the case of UPS 1307, a DC8 with an onboard fire, the crew ability exceeded the negative stressors and they successfully landed the aircraft in 2006. Yet four years later the crew of UPS 6 with a similar fire was overwhelmed and failed.
“The overwhelming” became the new hazard and became the reason for the mishap. It is not the individual items, no matter how important each sounds individually, in and of and by themselves.
They were just overwhelmed by events, overcome by events or OBE. They just could not stay ahead because they were faced with too much all at the same time. In the case of UPS 1354, if the weather actually had been 1000 overcast, they would have been fine. If the runway was the main ILS, they would have been fine. If there was not high terrain out there in the approach corridor, they would have been fine. If they were not so fatigued, they would have picked up in the errors and been fine. But when all of this is added together, it just overwhelmed them. The things going awry were not all hazards even, just unusual set of facts that collectively combined to swamp the crew.
3. Here is the third thing. When we were flying international, we often had a standards pilot, company check airman, training guy ride with us, often as once or twice a month. Part of it was that it seems just about every gateway airport has a unique procedure set that they use that no one else uses and is not written down anywhere. Or they have written set of procedures again unique, that you plan for, but that they do not use. The line check guys ride along it seemed, more to point out these peculiarities and discuss them with you, not so much to check you on it.
Flying Europe, the Americas and Asia routes, the check airmen’s insight was valuable and appreciated. The experience was always positive and two way, in our recollection. Okay, now here is the thing we have been leading up to. If the company could schedule all of these check airman flights and for good reason, why couldn’t they find a domestic flight with a heightened level of Unusuality, where the pilots are dead tired, the weather is down, the ILS is out, the terrain is rising, the copilot is new, the captain is doing his best, but so much is stacked up against the crew; why not just throw one of these check captains on the flight for the ride out early in the morning? Why not just add a third pilot, another set of eyes, someone to discuss with them a procedure that they seldom if ever use? What harm would it do?
If the company has enough check airmen, why not have them ready to ride when Unusuality is measured to be high on a particular flight? The company could have enough check captains to ride along with Unusuality indicated flight crew and point out the finer points of running the FMS through a discontinuity for a NP approach in the mountains, at night in the fog. Why not consider this? It would be good training and help overcome the huge clear case of Unusuality that could now be easy to see,
Some may say, “baby sittng.” But is it baby sitting in to have additional standardization flights or line observation flights? Which is cheaper, one check crewman or a crew, a plane and all lost in a mishap?
[1] http://en.wikipedia.org/wiki/Malcolm_Gladwell
[2] http://en.wikipedia.org/wiki/Malcolm_Gladwell
[3] YouTube.com. Miracle on the Hudson; https://search.yahoo.com/yhs/search;_ylt=A0LEVvvCTG1VP3oARUUnnIlQ;_ylu=X3oDMTEwNzJpNmJwBGNvbG8DYmYxBHBvcwMxBHZ0aWQDBHNlYwNyZWwtYm90?ei=UTF-8&hsimp=yhs-001&hspart=mozilla&fr=yhs-mozilla-001&p=miracle+on+the+hudson+audio&fr2=14166
[4] http://en.wikipedia.org/wiki/US_Airways_Flight_1549
[5] http://www.nbcnews.com/id/28678669/ns/us_news-life/t/ny-jet-crash-called-miracle-hudson/#.VW1NM6aUer8
In Summary:
Unusuality can be known ahead of a mishap because it is a comparison of facts known or knowable before a mishap occurs. This observation is the result of studying dozens of commercial airline mishap reports from NTSB, BEA and other mishap investigation agencies. Unusuality exists because the probable and contributing causes for mishaps combine to overwhelm crewmembers ability at the time of the mishap. Crew ability is also variable value, with changes coming from fatigue, training, crew resource management, communications ability, managerial ability, the ability to recognize negative stressors both individually and collectively in comparison to the crew’s current level of ability.
If Unusuality can be recognized, it can be recognized ahead of a mishap occurring if the commercial airline is able to create a metric using the seven principles listed herein. Lastly, if the Metric for Recognition of Unusuality is successful, it can be used to adjust local operational procedures to avoid the impact of the negative stressors on flight operations and prevent a mishap from occurring due to the overwhelming of the flight crew.
>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>>

CV: Captain David Williams served as an FAA designated check airman at a regional airline and as a line and training captain. He served as an aircraft mishap board member and as a pilot association safety representative. A US Navy career veteran from the maritime and antisubmarine patrol community, he served in numerous capacities in training, flight instruction and standards, including as a fleet pilot evaluator and check airman. Now retired from flight operations, Captain Williams remains active in safety and training issues. His goals have always been to train to the particular characteristics of each individual so that the pilot group as a whole is standardized and competent. He holds a degree in engineering and does consulting work in emergency response planning.
Captain Paul Miller is an international captain retired from a major global commercial airline. In pursuing the goal of flight operations with zero mishaps, he has served on the pilot association safety committee and on the joint safety forum of the association and the airline. He helped to compose the first rough draft of the FAA Advisory Circular on the joint FAA, airline and pilot association Aviation Safety Action Partnership (ASAP). He served as a safety program manager previously in the US Navy managing safety at two major air installations and a carrier based passenger and logistics squadron. He served on the European Advisory Committee, Flight Safety Foundation. He has presented papers on safety program management, safety forecasting, safety planning and response-based safety programs. He holds a degree in engineering from Rensselaer Polytechnic Institute, a minor degree in Humanities from Saint Leo University and has studied business administration at The College of William and Mary.

End Notes:
[1] http://en.wikipedia.org/wiki/Straw_that_broke_the_camel’s_back
[2] KPLR 11 (TV), St Louis, aired, “Amtrak Train thought to be…”, posted May 15, 2015 by CNN Wires, kplr11.com/2015/05/13/amtrak-train-thought-to-be-going-twice-as-fast-as-it-should-have-been/
[3] ibid
[4] Williams, Miller Study of Commercial Mishaps, 2015, published online at Safetyforecast.com
[5] Miller and Williams Predictive Mishap Recognition Using Unusuality Study, 2015, published online at Safetyforecast.com
[6] ibid
[7] ibid
[8] False Color, April 2000, published online at http://starchild.gsfc.nasa.gov/docs/StarChild/questions/question20.html
[9] http://www.referenceforbusiness.com/management/Str-Ti/Synergy.html
[10] http://www.referenceforbusiness.com/management/Str-Ti/Synergy.html
[11] Williams and Miller compilation of various AAR’s
[12] Fatigue Study showing mental alertness related to rest., http://www.utu324.com/?path=agreements/Union%20Docs/Fatigue%20Rest/FRF-002.pdf%3f
[13] Swiss Air 111 AAR, http://www.pbs.org/wgbh/nova/aircrash/dissection.html
[14] http://en.wikipedia.org/wiki/Swissair_Flight_111
[15] http://en.wikipedia.org/wiki/To_a_Mouse, poem by Robert Burns, 1785
[16] Crisis management: The Anatomy of an NTSB Investigation. A Guide for Parties to the Investigation and their Lawyers, April 2013, David Tochen, NTSB, Thomas Tobin, Wilson&Elser, New York.
[17] ibid
[18] FSF Proceedings, IASS 2014, Washington, DC.
[19] Statistical Summary of Commercial Jet Airplane Accidents 1959-2013, Seattle Washington, August 2014 http://www.boeing.com/resources/boeingdotcom/company/about_bca/pdf/statsum.pdf
[20] David Learmont, Flight International, Year in Review, EASS 2010, Lisbon, http://flightsafety.org/aviation-safety-seminars/european-aviation-safety-seminar/eass-proceedings/eass-2010-proceedings-contents
[21] FAR Part 121 Flight Training Curriculum Segments: http://fsims.faa.gov/PICDetail.aspx?docId=8900.1,Vol.3,Ch19,Sec6
[22] http://en.wikipedia.org/wiki/United_Airlines_Flight_232
[23] US Airways Flight 1549 NTSB/AAR-10/03 PB2010-910403 adopted May 4, 2010
[24] ibid, page 3
[25] “What is the Relationship Between Training and Safety in Commercial Air Operations?”, Miller and Williams, Flight Safety Foundation EASS Proceedings, Washington, DC, March 2010
[26] NASA Ames Research Center Fatigue Countermeasures Program, http://ntrs.nasa.gov/archive/nasa/casi.ntrs.nasa.gov/19950006379.pdf
[27] Wayne Rosenkranz, FSF, AeroSafetyWorld, http://flightsafety.org/aerosafety-world-magazine/sept-2012/top-level-automation
[28] NTSB Report: American Eagle Flight 4184
[29] http://www.bea.aero/en/enquetes/flight.af.447/rapport.final.en.php AF447 AAR, BEA, July 2012
[30] http://en.wikipedia.org/wiki/List_of_accidents_and_incidents_involving_the_Douglas_DC-8
[31] Williams and Miller Study, 2015, published at http://safetyforecast.com
[32] NTSB Report, USAir 1549, published 2010.
[33] NTSB Report, United 232, 1998
[34] Ethiopian Airlines B767(ET-AIZ) Aircraft Accident in the Federal Islamic Republic of the Comoros, in the Indian Ocean on November 23, 1996″ Ethiopian Civil Aviation Authority. 4 May 1998.
[35] http://en.wikipedia.org/wiki/Straw_that_broke_the_camel’s_back
[36] http://www.pbs.org/wgbh/nova/aircrash/dissection.html
[37] Aircraft Accident Report ASC-AAR-02-04-001: Crashed on a partially closed runway during takeoff Singapore Airlines Flight 006 Boeing 747-400, 9V-SPK CKS Airport, Taoyuan, Taiwan 31 October 2000,” Aviation Safety Council, Taiwan, Republic of China
[38] http://www.ntsb.gov/news/events/Pages/Runway_Overrun_and_Collision_Southwest_Airlines_Flight_1248_Boeing_737-7H4_N471WN_Chicago_Midway_International_Airport_Chi.aspx
[39] http://www.ntsb.gov/investigations/AccidentReports/Pages/AAR0201.aspx
[40] http://libraryonline.erau.edu/online-full-text/ntsb/aircraft-accident-reports/AAR96-01.pdf
[41] http://www.ntsb.gov/investigations/AccidentReports/Reports/AAR0502.pdf
[42] http://en.wikipedia.org/wiki/Icing_conditions
[43] http://www.aopa.org/News-and-Video/All-News/2005/August/1/Pilot-Counsel-(8)
[44] http://www.skybrary.aero/index.php/In-Flight_Icing
[45] http://libraryonline.erau.edu/online-full-text/ntsb/aircraft-accident-reports/AAR96-01.pdf
[46] http://www.ntsb.gov/investigations/AccidentReports/Reports/AAR9602.pdf
[47]https://books.google.com/books?id=nQZyAgAAQBAJ&pg=PA567&lpg=PA567&dq=resnick+super+cooled+liquids&source=bl&ots=_s3iRUA5x3&sig=DtbGRtWfZqI1rtL8DmKkbKR954c&hl=en&sa=X&ei=KO9lVfy7NMvSoATohICADg&ved=0CCoQ6AEwAw#v=onepage&q=resnick%20super%20cooled%20liquids&f=false
[48] ibid
[49] http://www.nasa.gov/centers/ames/news/releases/2004/humanfactors/humanfactors.html
[50]http://www.researchgate.net/profile/Kevin_Gregory2/publication/13535866_Flight_crew_fatigue_IV_overnight_cargo_operations/links/00b495283be32c56fe000000.pdf
[51] http://www.utu324.com/?path=agreements/Union%20Docs/Fatigue%20Rest/FRF-002.pdf%3f
[52] http://ntrs.nasa.gov/archive/nasa/casi.ntrs.nasa.gov/19950006379.pdf
[53] http://www.project-tenerife.com/engels/PDF/Tenerife.pdf
[54] http://en.wikipedia.org/wiki/Tenerife_airport_disaster#Probable_cause
[55] ibid
[56] http://www.project-tenerife.com/engels/PDF/alpa.pdf
[57] http://www.ntsb.gov/investigations/AccidentReports/Pages/AAR1001.aspx
[58] http://www.ntsb.gov/investigations/AccidentReports/Reports/AAR0102.pdf
